


Puberty is the period when the body develops from child to adult. Puberty usually starts between the ages of 10 and 13, but the timing of its onset can vary considerably. Some people begin puberty early and for some it occurs a number of years later. An individual cannot influence the onset of puberty themselves. Girls usually begin puberty between the ages of 8 to 13 and boys around the ages of 11 to 15. Puberty usually lasts for 4 to 6 years and during this period changes occur at different rates. Puberty is finished when an individual is fully grown.
Exercise and training are good for children’s and young people’s well-being. It is important that training and exercise is varied and that it includes mobility, strength, balance and endurance. In order to get the most out of training, and to ensure that training does not harm the body, it is extremely important to eat a versatile diet and consume as much energy as is burnt via the combination of exercise and growth. The most important meal is the one immediately after exercise.
Growing children need a lot of carbohydrates and young athletes, naturally, need even more!
Common causes of developing overload injuries in children and young athletes are consuming too little energy and performing repetitive and unvaried training. In other words, you should load just right, at the right frequency and with variety and consume as much energy as you burn, plus a little extra so that the body can grow.
Growth spurt
The skeleton grows from birth until around the age of 13 to 15 years old for girls – depending on the onset of puberty. For boys, the skeleton grows over a longer period; until they are 16 to 19 years old. The growth spurt, that is, the roughly 3 months in which a child grows extraordinarily quickly, often occurs for girls shortly after they have had their first period and for boys sometime later in their teens. In this period a child grows very fast over the course of a few months. The growth spurt begins with the feet and hands, this is followed by growth of the arms and legs and finally with growth in the spine.
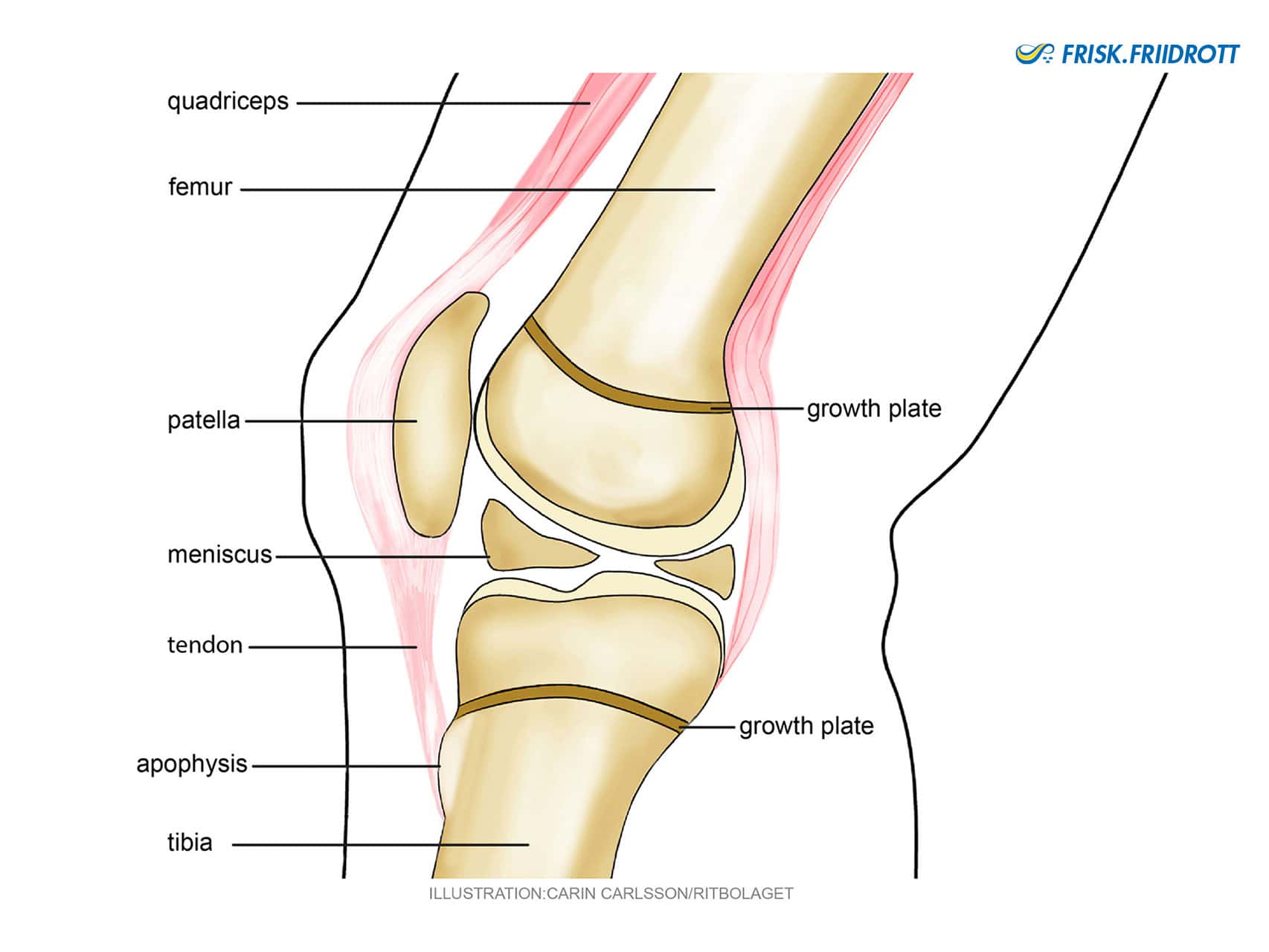
Growth plates – are the area where the bones grow. These plates consist initially of cartilage that produce bone cells and they become bone when fully grown. The growing skeleton has open growth plates that are not sufficiently mature to tolerate the same type of loads that a fully-grown skeleton can. For example, repetitive high loads may increase the risk of slipping in a growth plate. The growth plate in the knee, for example, closes around the age of 20. Common growth-related disorders that many young athletes experience are those that affect the heels and knees, you can read more on these issues in the section on common injuries in youth sports.
Active growth plates in various bones and their approximate ages of closing:
- Feet 14-21 years old
- Heels 12-22 years old
- Ankles 16-18 years old ‘
- Knees 16-19 years old
- Hips 16-18 years old
Apophyses – are bony tubercles, which are close to the bone growth zone, where muscles & ligaments attach or originate.
What to consider when coaching young athletes who are growing
It is important that exercise and the structure of training reflect the biological age of the young athlete, i.e. their physical maturity, and not their chronological age (which is years from birth).
The long bones (e.g. those in the arms and legs) grow at a slightly faster rate in comparison to the surrounding muscles. This can mean that, during periods when the bones grow, different levers and higher loads can occur at apophyses, i.e. the area where the muscle tendons attach to the bones. It is also the case that when children and young people grow, much of the growth occurs around the apophysis. Therefore, during training these areas can be overloaded and cause issues such as Sever’s and Osgood-Schlatter’s diseases.
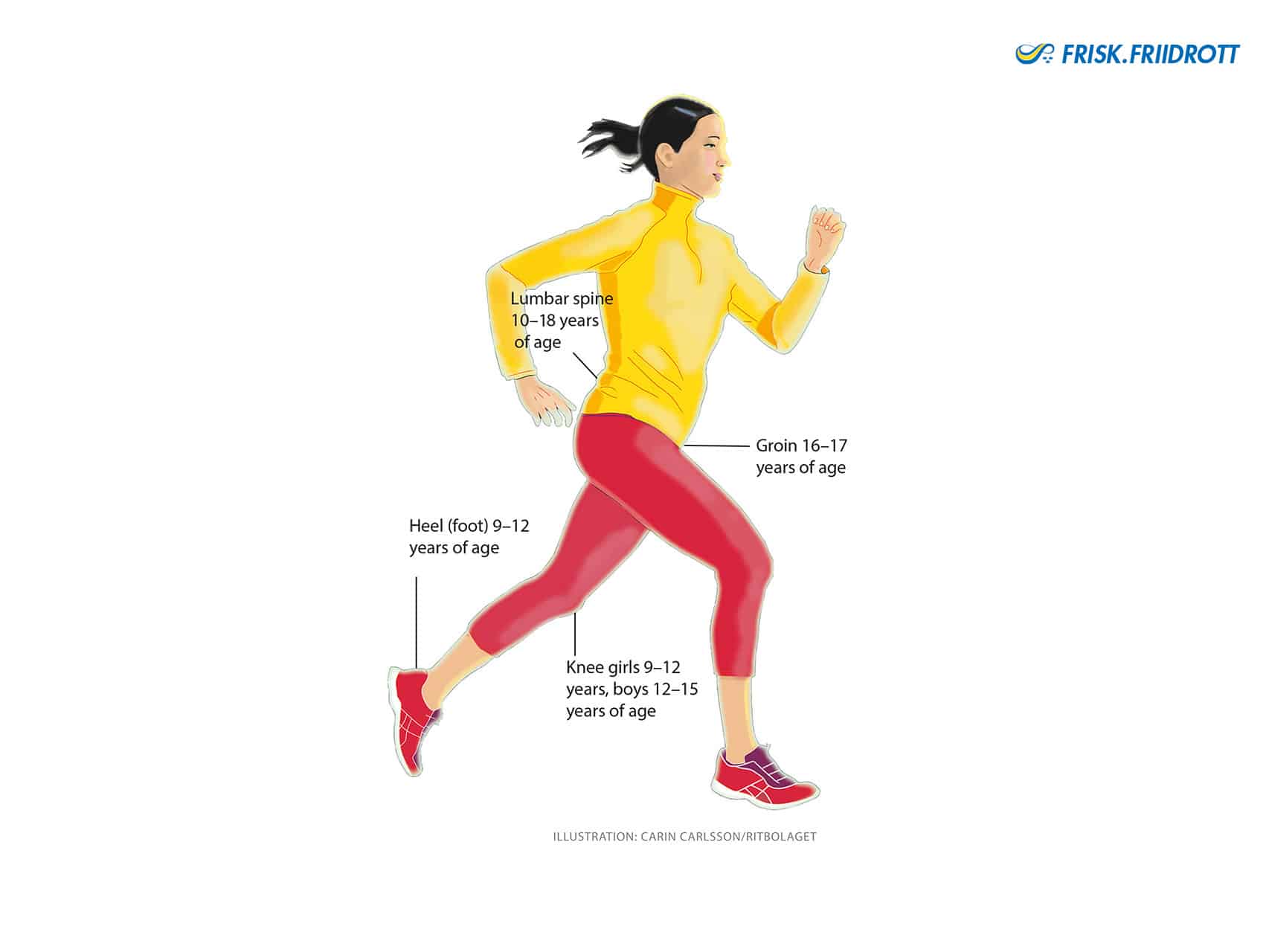
We grow in different phases and common problems / “injuries” in young athletes usually follow a pattern that begins at the bottom and works up the body;
- Feet (and hands) grow first. This happens around 9 – 12 years of age and can cause pain in the heels, so called Sever’s disease. It is not uncommon for many young people to feel that “I have such large feet!” But try to remain calm, the rest of the body will catch up! 😃
- In the next phase the arms and legs grow. This happens around 9-12 years of age for girls and 12-15 years of age for boys. This can lead to young athletes developing pain in their knees, so called Osgood-Schlatter’s disease.
- Groin problems usually occur around 16 – 17 years of age. Loading-related pains usually affect the area around the muscle to bone attachments (apophyses) in the groin.
- The lumbar spine undergoes a rapid growth that begins around the age of 10 and continues up to 18 years of age. During this period, the lumbar spine grows about 3 cm!
It is not uncommon for young people who experience symptoms related to growth to also experience a pattern – first they get issues with their heels, then the knees and then perhaps issues with the groin (usually in boys) and lumbar spine (slightly more common among girls). The vast majority of these conditions improve (disappear altogether) when that area of the body has finished growing. When planning training, you can consider what type of exercise increases loading in the growing area and attempt to reduce (remove) this type of exercise for a period of time before gradually reintroducing it.
Be aware that growth in the knees, groins and lumbar spine often occurs at an age when many young athletes start to train and compete at an elite level!
It is therefore particularly important to vary training loads, and it is preferable to reduce exercise for a week than to continue with pain and risk prolonging issues. For more specific information on how these complaints should be managed see the section on common injuries in youth sports.
During the growth spurt, all of the body’s joints are very sensitive to loading. Therefore, during this period types of training that heavily load the joints should be reduced, e.g. avoid too much explosive jumping and bounding and do not train with heavy weights. These three months can be used to focus on mobility, aerobic and technique training! Heavy loads on the joint surfaces can cause lifelong cartilage damage.
Question
How do I know if a child is undergoing a growth spurt? Unfortunately, it is not possible to perform any simple tests to confirm this, but it can be beneficial to ask parents or guardians to keep track of how much their child grows, in terms of height, for example, by measuring them every 3 months.
When a young person grows, and when they have just finished growing, i.e. when they are noticeably taller and perhaps have increased in weight, they will have new levers & loads that need to be taken into account in their training!
Bones are strengthened when they are loaded in several different directions! Loading affects bone density and skeletal mineralisation increases up to the age of 20-25. Early specialisation, with unilateral (one-sided) movement patterns, is not good for bone health!
Three keywords to remember concerning optimal bone health are: periodisation, variation & recovery.
References and further reading:
Behrooz A. Akbarnia, Muharrem Yazici, George H. Thompson, editors. The Growing Spine: Management of Spinal Disorders in Young Children. Heidelberg ; New York : Springer. 2016.
Handbook of Sports Medicine and Science: The Female Athlete. Editor: Margo L. Mountjoy MD, © 2015 International Olympic Committee. Print ISBN:9781118862193. 2015. The Female Athlete_Mountjoy.pdf
Peterson L, Renström P. Sports Injuries. 4ed. Taylor and Francis. 2016.
Svensk Friidrott. Grundträning I friidrott 10-14 år. SISU idrottsböcker. 2013.
Thomeé R, Swärd L, Karlsson J. Nya Motions- och idrottsskador och deras rehabilitering. SISU Idrottsböcker. 2011.
Wikström-Frisén L, Nordström A. Kvinnor och träning. SISU Idrottsböcker. 2017.
Sverker N – Sports Medicine Physician, PhD. Chair of The Medical Committee Swedish Athletics.
Scientific publications